Indian Journal of Physiology
and Pharmacology
and Pharmacology
Indian Journal of Physiology and Pharmacology |
 (252x320).jpg) |
Volume 58 - Number 2 April - 2014 (Current issue) ISSN 0019-5499 |
Effect of Gender and Body Mass Index on Pulmonary Function Tests in Adolescents of Tribal Population of a North Eastern State of IndiaDipayan Choudhuri, and Soma Choudhuri |
The present study was planned to assess the pulmonary function in tribal adolescents (age 12-16 yrs) of Tripura, a north eastern state of India, and to evaluate the effect of body mass index (BMI) on pulmonary functions of male and female subjects from tribal population. One hundred and seventeen male and seventy female subjects were selected for the study through a randomized method of sampling. Pulmonary function parameter recorded were forced vital capacity (FVC), forced expired volume in 1 second (FEV1), peak expiratory flow rate (PEFR) and maximal expiratory pressure (MEP). Values of all the pulmonary function parameters recorded in female subjects were found to be lower than the male subjects. FVC, FEV1, PEFR, MEP recorded in subjects from both the sexes correlated significantly with BMI. The results of the study provide basic data on pulmonary function parameters of tribal adolescents from Tripura. |
Pulmonary function is known to vary with age, sex,
race, ethnicity and geographical location of the
subject (1). In addition, lung function is associated
with height, weight and body mass index of the
subject after adjusting for other factors such as
age, race, sex, asthma and smoking status in
populations that are at risk for reduced lung function (2, 3). India, being a subcontinent, changes in
pulmonary function can occur between children of
different region and race (4). Studies involving different
tribes of India revealed existence of ethnic differences
among the tribal of the country in terms of their
nutritional and other health parameters (5). No
previous study has provided data on pulmonary
function parameters on randomly selected healthy
adolescents from tribal population of Tripura. With
this purpose, we evaluated various anthropometric,
physiological and respiratory parameters in
adolescent male and female children from
tribal population of Tripura. Correlation between
body mass index and respiratory parameters of
the subjects from both the sexes were also
evaluated. |
The study was conducted on 187 randomly selected school children of both sexes aged 12 to 16 years from tribal population of Tripura. 117 of them were male and 70 were female. Only healthy non-smoking students without any respiratory, neuromuscular, cardiac and endocrine disorders were included in the study. Institutional ethical committee approved the protocol of the study. Consent to participate in the study was obtained from parents of each student. Age (yr), standing height (cm), body weight (kg), chest circumference (cm), mid upper arm circumference (cm), waist - hip ratio were measured using standard procedure (6). Height was measured to nearest of 0.1 cm and weight was measured to nearest of 0.1 kg. Chest circumference was recorded both during normal respiration and maximal expansion at the end of inspiration. Waist circumference measurements were made by positioning the tape between coastal margin and iliac crest of the subject. Body mass index was calculated by formula from height and weight of the subject (7). Physiological parameters recorded included resting heart rate, respiratory rate and blood pressure. Forced Vital capacity (FVC) and forced expiratory volume during 1st second of expiration (FEV1) were recorded according to American Thoracic Society (ATS) guidelines (8) by using an expirograph (Helios 401, RMS, and India). Peak expiratory flow rate (PEFR) was recorded by using Wright’s peak flow meter. Maximal expiratory pressure (MEP) of the subject was recorded by using a modified Black's apparatus by expiration from total lung capacity after a maximal expiration in sitting posture in empty stomach. The pressure was sustained at maximal force for at least one second. The manoeuvre was repeated for three times with one minute interval between repetitions. The highest value was accepted for computation (9). All parameters were recorded during morning hours
7.30am to 9.30am to minimize possible diurnal
variation. First, the manoeuvres were demonstrated
and then the subjects were asked to perform the manoeuvre. Maximum of eight trials including the
final readings for each manoeuvre was allowed. All
the respiratory measurements were taken after
placement of nose clip. All the values were presented
as mean+SD. Level of significance was assessed by
using unpaired student's t test. Linear association
were established by using Pearson's correlation. The
statistical analysis was performed using software
SPSS version 19.0. |
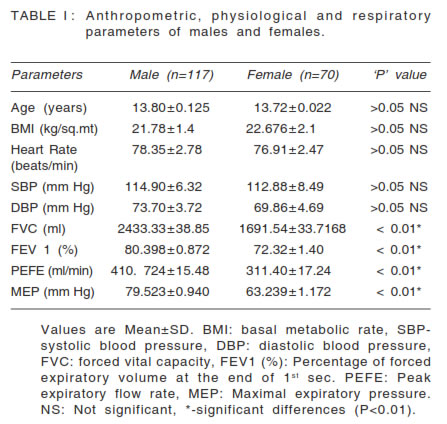
Values of various anthropometric, physiological and
respiratory parameters recorded in both male and
female subjects are presented in Table I. All the
parameters including BMI are within the normal range
for the age and sex of the subjects. Blood pressure
and heart rate of the subjects are within the normal
range. Respiratory parameters like VC, FEV1 and
PEFR and MEP are found to be significantly lower
in female subjects in comparison to male subjects.
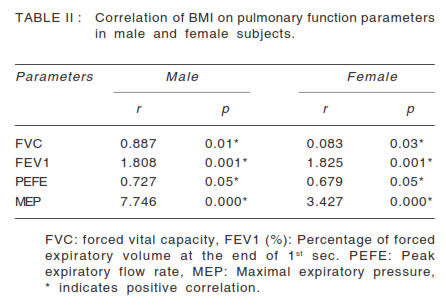
The correlation of different pulmonary function
parameters with BMI of the subjects are presented
in Table II. It is observed that parameters like FEV,
FEV1, PEFR and MEP of the subject correlated
positively with BMI. |
 |
 |
This study determines the normal values of lung function in tribal adolescents of Tripura, a north eastern state of India, who are in the age group of 12-16 years. The aim of the study was to see the correlation of different lung functions parameters with BMI in both male and female subjects. While comparing the lung function parameters in different sex groups it has been observed that lung function values are more in male in comparison to the female subjects. These results were comparable with the study done by Rajkapoor et al in which they found that mean lung function test was higher in boys than in girls except FEF50%, FEF75% which were higher in girls. Budhiraj et al. also reported lower pulmonary function values in female than the male subjects in similar age group (10). The sex difference in lung function may be attributed to various factors including of sex hormone, sex hormone receptor, or intracellular signalling pathway in addition to physiological and anatomical differences in respiratory system of male and female (11, 12). Measurement of lung volumes is important components of pulmonary assessment in children and adolescents with lung disease. Many physical factors that are correlated with pulmonary function are height, weight, sex, arm span and body mass index (13). Body mass index (BMI) is considered to be the best variable for anthropometric evaluation in nutritional and the general health screening (14). Many of the studies all over the world have correlated pulmonary function parameters with BMI of the subject (15, 16). These studies revealed there is definite correlation between BMI and pulmonary function parameters. Thyagarajan et al. have observed, among healthy adults, increasing BMI in the initially thin participants was associated with increasing than stable lung function through age, but there were substantial lung function losses with higher and increasing fatness (17). In our study we have observed a positive correlation in all the lung function parameters studied with BMI of the subject. This can be explained by the fact that all our subjects are within the normal range of BMI for their age and sex. These observations are in agreement with several cross sectional studies that found association of FVC and FEV1 with baseline BMI (18, 19). However, gain in BMI or body fat is found to be related to longitudinal decline in FEV1 and FVC in general population (20, 21). Our study has not evaluated effect of longitudinal changes of body mass index on pulmonary function. Like FVC and FEV1, maximal expiratory pressure (MEP) in different groups of population is found to be influenced by biotype, anthropometric characteristics, nutritional status and physical fitness of the subject (22). MEP, in our study, is found to be positively correlated with BMI of the subjects in both the sexes. The influence of BMI on MEP may be explained due to increase in muscle mass in subjects with higher BMI (23). In conclusion, the value of various pulmonary function parameters obtained in the present study for a sample of 12 to 16 years old children from tribal population of Tripura are comparable with reported values on children from other region of India. Given the lack of available reference values in the study population, this study may be considered an important guide to researchers as to suitable parameters for assessing pulmonary function in this group of children. However, it is also important to note that further studies are still necessary, involving greater sample of subjects including a wide age and socioeconomic range from various regions of Tripura. |
|